After undergoing surgery on the stomach, large intestine, appendix, liver, gallbladder, pancreas, uterus, and ovary, the intestines, the intestines, and abdominal wall stick together, causing peritoneal adhesions. Postoperative adhesions occur at a rate of 65-95% and can cause adhesive bowel obstruction leading to chronic pain. When the abdominal wall is damaged by surgery, plasma containing a large amount of fibrin, a protein that tries to repair the wound. Also, leukocyte exudation related to inflammation and the protein, fibrin cause blood clots known as hemostasis. However, it is a biological mechanism necessary for tissue repair. Due to this physical mechanism, excessive tissue leakage of fibrin is known to cause inflammatory fibrosis and adhesions.

Yet, no helpful method has been established to prevent postoperative adhesions. On the other hand, in recent years, it has been reported that fucoidan, a sulfated polysaccharide obtained from brown algae, inhibits the formation and fibrosis of fibrin clots in addition to its anti-inflammatory effect.
Therefore, in this blog, the study “Fucoidans inhibit the formation of postoperative abdominal adhesions in a rat model,” by Alex J. Charboneau et al., I would like to share how fucoidan was administered into the abdomen of rats and prove the effect of fucoidan administration related to the suppression of postoperative abdominal adhesions by measuring tissue pathology and blood coagulation parameters.
First, a 2.2×2.5 cm cut was excised from the abdominal wall of Sprague Dawley (SD) rats to create an adhesion model. Peridan, a formulation containing fucoidan reagent derived from Fucus Vesiculousis (kelp family SFC) and kelp extract, was used in this test. SFC was administered at 4.3, 8.3, 17.2 mg/day and Peridanga 5.3, 10.6 mg/day, respectively, to the abdomen using an osmotic pump for seven consecutive days. The effect of fucoidan administration on adhesions was compared with the control. The results were evaluated by quantifying the extent of adhesions on the subcutaneous surface and calculating a unique adhesion score. (Fig. 1)
As a result, it was found that continuous administration of SFC and Peridan significantly lowered the adhesion score. Adhesions were also considerably reduced when a single dose of SFC (80 mg) was administered. Finally, to evaluate the systemic anticoagulant effect of fucoidan, systemic coagulation parameters, International Normalized Ratio (INR), and Activated Partial Thromboplastin Time (aPTT) is an index indicating the speed of blood coagulation reaction, was measured. aPTT indicates intrinsic coagulation by intracellular blood factors, and INR indicates extrinsic coagulation by tissue factors. The higher the value, the stronger the anticoagulant effect.
Intraperitoneal administration (50mg) of Peridan caused a rapid increase in aPTT, which decreased to almost basal lows within 5 hours after that. In addition, it was clarified that both Peridan and SFC have the same level of effect as warfarin (antithrombotic drug) treatment which has a maximum INR value of about 2 to 3 (Fig. 2). Thus, this study clarifies the effectiveness of fucoidan in suppressing postoperative adhesions and is expected to be helpful as a therapeutic means for future postoperative management.
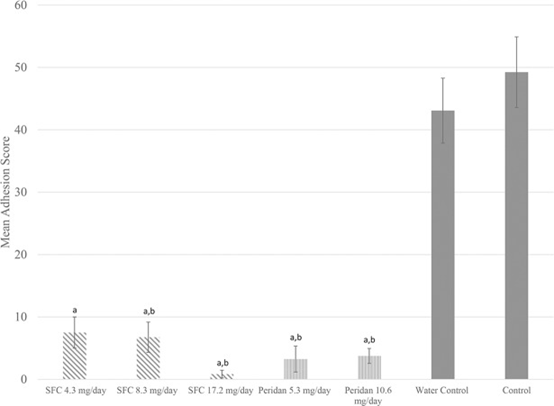
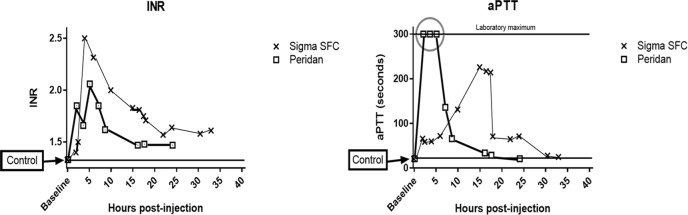
Fig.2)Fucoidan effect on coagulation factors