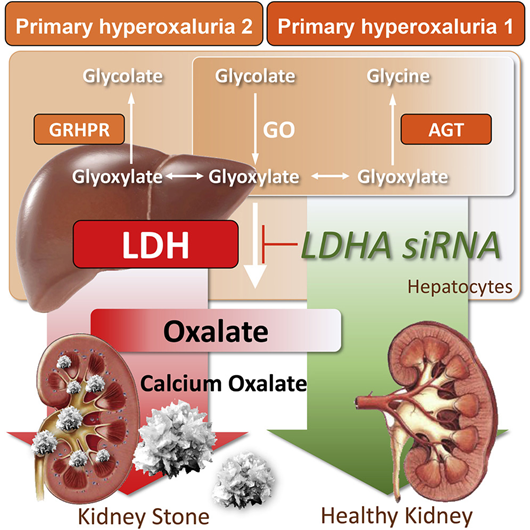
Primary hyperoxaluria is caused due to congenital deficiency of metabolic enzymes, a disease in which the liver overproduces oxalic acid. Overproduced oxalic acid causes stones and calcification in the kidney, gradually impairing kidney function. If it progresses further, it leads to end-stage renal failure. Thus the person suffering from this disease is forced to undergo dialysis. In addition, when kidney function declines, it begins to deposit in organs throughout the body such as bones, heart, blood vessels, and retina of the eye, causing various disorders.
Treatments include remedies used for treating stones, but they also have side effects such as gastrointestinal disorders. On the other hand, fucoidan, a sulfated polysaccharide, is a natural ingredient and a supplement that has no side effects.
In this blog, I will present the effect of fucoidan on hyperoxaluria based on the research contents of “Physico-chemical alterations of urine in experimental hyperoxaluria: a biochemical approach with fucoidan” by Coothan Kandaswamy Veena et al.
First, dividing two groups of male albino Wistar rats (120 ± 20 g) were given 0.75% ethylene glycol (EG) for 28 days to induce hyperoxaluria, one of which was a sulfated polysaccharide (Fucoidan from Fucus vesiculosus, 5 mg kg-1, sc) was administered. One group was maintained as the regular control group. The other group served as drug controls administered with sulfated polysaccharides. Urine collected from all groups was analyzed for changes in pH, volume, oxalate, calcium, phosphorus, uric acid, magnesium, citric acid, and glycosaminoglycans, in addition to examining urine crystals by light microscopy.
Kidney tissue was studied under polarized light for crystal deposition, and their oxalate and calcium content was analyzed. Changes in the extracellular matrix during crystal deposition were also evaluated. As the weight of the kidneys increased, the pH and volume of urine in EG-treated rats changed. In addition, administration of EG to rats increased levels of stone-forming components such as oxalate, calcium, phosphorus, and uric acid and increased urinary supersaturation. It was entirely recovered by fucoidan treatment.
The reduction of inhibitors such as citrate, magnesium, and glycosaminoglycans in urine was prevented by combination treatment with fucoidan. Furthermore, high calcium oxalate rats had increased excretion of calcium oxalate monohydrate.
Crystals in the urine and crystal deposits in kidney tissue were prevented by fucoidan treatment (Fig.1). Administration of fucoidan even reversed tissue levels of calcium and oxalate. In addition, increased collagen accumulation and transforming growth factor-β1 expression in hyperoxaluria was normalized by fucoidan administration. These results suggest that the physicochemical changes in urine produced during hyperoxaluria can be reversed by fucoidan administration.
A B
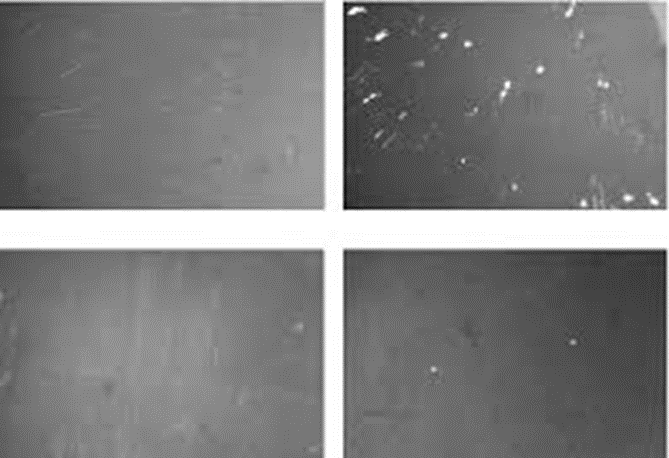
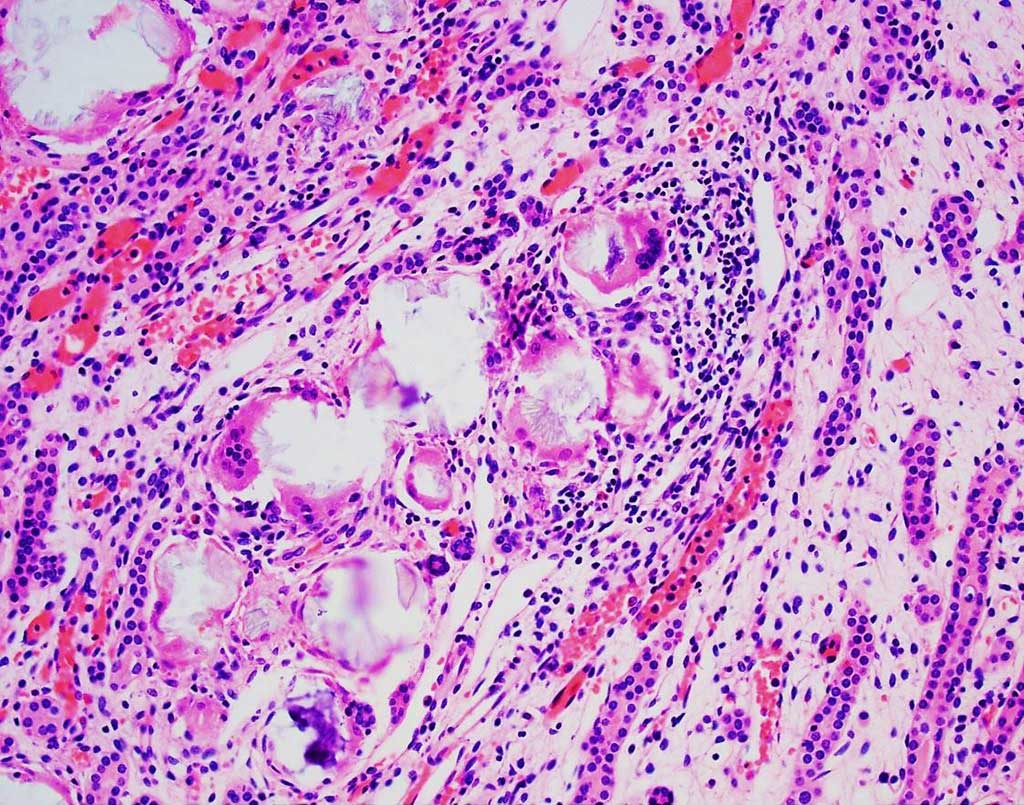
Fig.1) Urine in experimental hyperoxaluria of a biochemical approach with fucoidan
A. Sections from control rats showing no crystals deposition. B. Sections from EG-treated rats showing the presence of aggregated crystals. C. Sections from fucoidan-treated rats show no crystal deposition. D. Sections from EG + fucoidan-treated rats show the presence of tiny crystals.