
Cancer is one of the leading causes of death globally across different age groups. The worldwide research to prevent cancer and offer treatment has already been underway due to its high incidence, morbidity, and mortality. While the research is still ongoing, fucoidan has been reported to have multiple positive functionalities such as anti-cancer effect and serum fat improving impact. As for the cancer effects, fucoidan mainly acts by inducing apoptosis, exhibiting the cell cycle, and inhibiting cell migration.
So, in this blog, I’ll be explaining how fucoidan induces apoptosis in colorectal cancer (HT29) by a different approach via the activation of DR4 and mitochondrial pathway. Although I have already discussed colon cancer in the previous article, it will offer a little more explanation of the study.
The colon is part of the body’s gastrointestinal system. The gastrointestinal system is responsible for the digestion and absorption of dietary nutrients such as vitamins, minerals, carbohydrates, fats, proteins, water, and eliminating waste products from the body. Currently, colon cancer is increasing rapidly among other cancer types. For example, if you overeat animal fat, you will secrete a lot of bile acids to help digestion. Unfortunately, bile acids that have moved to the large intestine are converted to “secondary bile acids” by harmful bacteria. Since this secondary bile acid contains carcinogens, it is considered as one of the causes of cancer in the mucous membrane of the large intestine.
First of all, I would like to inform you of the research by “Fucoidan Induces Apoptosis of HT-29 Cells via the Activation of DR4 and Mitochondrial Pathway” by XU Bai et al. to investigate the effect of fucoidan on colorectal cancer cells. They used 100-800 µg / mL of Fucus vesiculosu-derived fucoidan as human-derived normal cells 293T and cancer cells (colon cancer cells HT29, breast cancer cells MCF-7, cervical cancer). It was added to cells (HeLa), and the viability of the cells was measured. As a result, the survival rate when fucoidan was added to normal cells was 100%.
In contrast, fucoidan showed a concentration-dependent effect on various cancer cells and was treated with 800 µg / mL fucoidan. The viability of HT29 cells was reduced to 40% (Fig. 1). Additionally, the involvement of cell death receptor 4 (DR4) expression in the induction of apoptosis by fucoidan was subsequently investigated. The expression level of DR4 increased in a fucoidan concentration-dependent manner, suggesting that DR4 may be required for the induction of apoptosis by fucoidan. Furthermore, to determine whether DR4 is required for inducing apoptosis of HT29 cells by fucoidan, siRNA was used to inhibit the expression of DR4. Finally, fucoidan was added to measure the viability of HT29 cells. As a result, under fucoidan 800 µg / mL condition, HT29 cells increased from 40% to 75% (Fig. 1 and Fig. 2). It indicates that fucoidan induces apoptosis of HT29 cells by activating DR4.
To determine whether the mitochondrial pathway activates HT29 cell apoptosis by fucoidan, we evaluated a decrease in mitochondrial membrane potential and cytochrome C expression. As the fucoidan concentration increased, it was confirmed that the internal mitochondrial membrane potential decreased, and its permeability increased. It is also proved that the release of cytochrome C from mitochondria to the cell membrane activates caspases that lead to apoptosis. In this study, the release of cytochrome C associated with the addition of fucoidan was confirmed (Fig. 3). These results indicate that fucoidan induces apoptosis through both the DR4-mediated and mitochondrial pathways. This study identified the activation mechanism of fucoidan-induced apoptosis-inducing pathways and provided the basis for the clinical application of fucoidan.
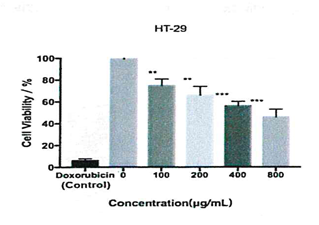
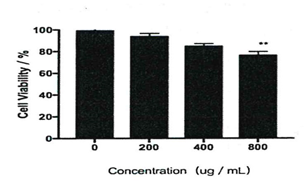
Fig. 2) Survival rate of colorectal cancer cells when DR4 is inhibited

Fig. 3) Amount of cytochrome C released from mitochondria